The Future of Scoliosis Surgery

Why Motion Preservation Matters
For decades, the standard surgical treatment for scoliosis has been spinal fusion surgery. Fusion has helped thousands of patients by stabilizing the spine and preventing curves from worsening. It remains one of the most reliable tools surgeons have for treating severe scoliosis.
But as pediatric spine care evolves, many physicians and researchers are asking an important question:
Can we treat scoliosis while preserving more natural spinal motion?
The answer may define the future of adolescent idiopathic scoliosis treatment.
The Challenge with Traditional Spinal Fusion
Spinal fusion works by permanently joining segments of the spine together using rods, screws, and bone graft. Over time, the fused vertebrae grow into a single solid structure.
The goal is straightforward: Stop the curve from progressing and restore spinal alignment.
For many patients with large curves, fusion remains the most appropriate treatment. However, fusion also comes with an unavoidable tradeoff, loss of motion in the fused portion of the spine.
For most patients, this loss of mobility does not significantly impact everyday life. Teens who undergo fusion often return to school, sports, and active lifestyles. Still, the idea of permanently eliminating motion in part of a young person’s spine has led surgeons to explore alternatives to spinal fusion for scoliosis.
Why Motion Preservation Is Important
The human spine is designed to move. Every time we bend, twist, run, or jump, multiple segments of the spine work together to distribute forces and maintain balance. When segments of the spine are fused, that movement no longer occurs in the treated area. Instead, adjacent levels take on additional mechanical stress. Preserving natural motion, especially in athletes or high activity patients, has become an increasingly important goal in scoliosis care.
Motion-preserving approaches aim to:
- Maintain spinal flexibility.
- Preserve natural biomechanics.
- Reduce long-term stress on adjacent spinal segments.
- Allow patients to maintain full physical activity.
These goals have fueled interest in non-fusion alternatives to scoliosis surgery.
The Rise of Motion-Preserving Scoliosis Treatments
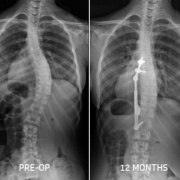
Over the past decade, new surgical techniques have begun to challenge the idea that fusion is the only option for correcting scoliosis curves. These approaches fall under the broader category of scoliosis surgery alternatives, which aim to correct or control the spinal curve while preserving mobility. One widely discussed comparison in the field today is vertebral body tethering vs spinal fusion.
In motion-preserving techniques like vertebral body tethering, the spine is guided into a more balanced alignment using tension rather than rigid fixation. As the child grows, the tether helps modulate spinal growth and gradually improve the curve. Instead of locking the spine in place, the goal is to guide the spine while allowing it to remain mobile. This represents a fundamental shift in thinking about scoliosis treatment.
A Changing Philosophy in Pediatric Spine Surgery
Historically, the primary objective of scoliosis surgery was to stop curve progression. Today, surgeons are increasingly thinking about long-term spinal function, not just curve correction.
This shift mirrors trends seen in many areas of orthopedics.
For example:
- Joint replacement has evolved toward bone-preserving techniques.
- Sports medicine emphasizes restoring natural biomechanics.
- Pediatric orthopedics prioritizes growth-friendly treatments.
In scoliosis care, this philosophy is leading to growing interest in motion-preserving solutions.
The Importance of Patient Selection
While motion-preserving treatments are exciting, they are also not appropriate for every patient.
Factors that influence whether a patient may qualify for non-fusion scoliosis surgery include:
- Curve size and flexibility
- Remaining skeletal growth
- Curve pattern and location
- Overall spinal balance
Some curves, particularly large or rigid ones, are still best treated with spinal fusion surgery for scoliosis. The goal is not to replace fusion entirely, but to expand the range of scoliosis treatment options available to patients.
What the Future May Look Like
The future of scoliosis surgery will likely involve a broader spectrum of treatment approaches.
Rather than a single solution, physicians may increasingly tailor treatment based on the patient’s age, growth potential, and curve characteristics.
Possible directions for the future include:
- More refined motion-preserving implant technology.
- Advanced biomechanical modeling to personalize treatment.
- Earlier intervention strategies designed to prevent severe curves.
As research continues, surgeons will gain a better understanding of which treatments provide the best long-term outcomes.
Expanding Options for Families
For families navigating adolescent idiopathic scoliosis treatment, the most important takeaway is that scoliosis care continues to evolve.
Spinal fusion remains the most common and most studied treatment option for many patients. At the same time, ongoing innovation is creating new possibilities that may preserve motion while still correcting spinal deformity.
Ultimately, the future of scoliosis treatment may not be defined by a single procedure, but by the ability to match the right treatment to the right patient at the right time. For young patients facing decades of activity ahead, preserving spinal motion whenever possible may play an increasingly important role in shaping the next generation of scoliosis care.